1. Importance of gender considerations for achieving health and nutrition outcomes for women and girls
Health is one of the key indicators of economic development of a family, community and nation. In addition to genetical conditions of individual or communities, economic status/poverty, availability and accessibility to quality health care services and resources, environment, and the social/community context are major determinants of health and nutrition outcomes (WHO). Gender disparity and gender inequality lies at the root of all these factors that causes differential/poorer health conditions of women, girls and children. There is ample evidence to inform the prevalent difference of health and nutrition outcomes between boys and girls or women and men. However, there is a major evidence gap to inform the impact of social/gender norms on the negative health status of women and girls. The role and influence of elements of her eco-system across her life cycle is also a critical gap area.
Despite India’s progress in reducing child mortality , the benefits thereof have not been equally shared by the male and female child. According to the ‘Levels and Trends in Child Mortality’ report’ by the United Nations Inter-agency group for child mortality, fewer nations showed gender disparities in child mortality, & across the world, on average, boys have a higher probability of dying before reaching age-5 than girls. But this trend wasn’t reflected in India. India is among the few countries in the world where, the mortality under-5 years of girls, exceeded that of boys. This means that girls have a higher probability of dying before attaining the age of five years than boys. Through backward deduction, this means that effects of malnutrition are more pronounced for girls than boys . The root cause of such male-female differentials is the socio-cultural practices and mindset of the people which contribute to continued widespread prevalence of gender discrimination. Understandably, reducing the prevalence of malnutrition among girls holds the key to reducing the burden of female under-five deaths. Research shows that the girl child experiences mistreatment and neglect from the time of birth and thereafter during early childhood, facing a disadvantage in accessing nutrition and is thereby exposed to a higher risk of morbidity and mortality. Based on analysis of differential treatment of girls and boys in North India, Barbara Miller terms the prevailing anti-female bias as extended infanticide in her book ‘The Endangered Sex: Neglect of Female Children in Northwest India’.
Differential gendered treatment of boys and girls, impact their health (physical, emotional, social, spiritual and intellectual) and overall social upbringing negatively. Social norms of restricted and controlled environment of upbringing severely truncates their growth and development as a healthy holistic human resource. High degrees of morbidities start during adolescence. As per WHO, most of the adult life mental health disorders start at the age of 14, which go undetected and untreated. Iron deficiency anemia is one of the top causes of years lost by adolescents. Unhealthy food and nutrition availability and habits are foundation to sick adulthood for these adolescents. In all such situations, girls are further disadvantaged due to their weaker and lower social status.
Adult female members of the household also tend to be treated as inferior and receive a relatively lower share of nutrition and economic resources. In this context, maternal nutrition has significant carry-over costs as well. Undernourished girls grow up to become undernourished mothers and give birth to potentially undernourished, low-birth-weight children, who are more susceptible to death and disease. In fact, this potentially explains why India has the largest incidence of low-birth-weight children globally. If this inter- generational self-perpetuating cycle is not broken, the problem of malnutrition would continue to fester.
Multiple studies have also shown that the predicament of women is more pronounced for low-income households with strong ‘son’ preferences and a greater prevalence of gender-bias. Women in households continue the practice of eating last and leftovers , have little say in purchasing decisions of the households, limited access to mobility and therefore avail timely health services, and the list is long…. contributing to their poor health and nutrition status.
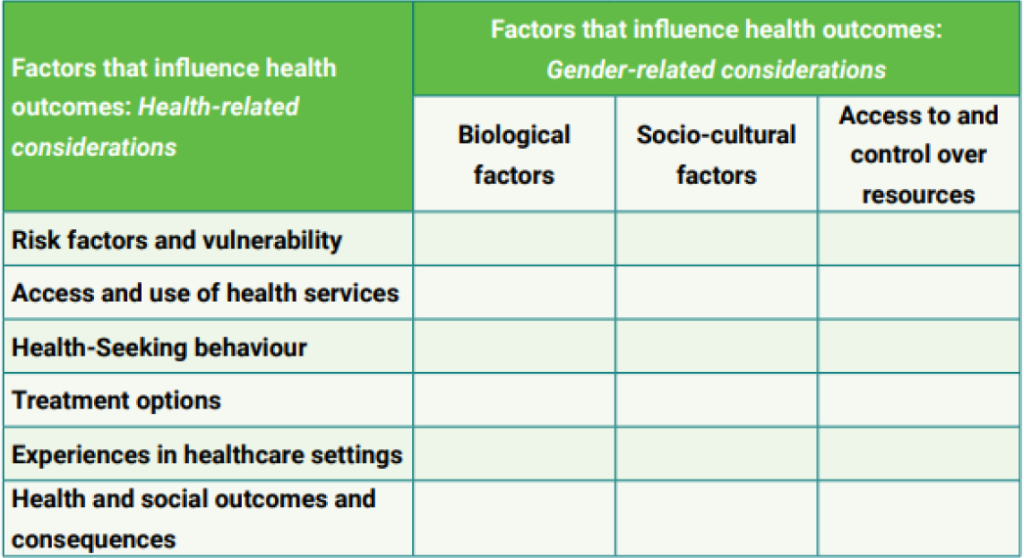
Gender norms, socialization, roles, differentials in power relations and access to and control over resources contribute to differences in vulnerabilities and susceptibilities to illness, how illness is experienced, health behaviours (including health-seeking), access to and uptake of health services, treatment responses and health outcomes.
Gender roles and barriers owing to gender norms and other stereotypes have been put into certain frameworks by many agencies that guide program design and are used for various gender analysis and behaviour change frameworks and models. Two examples of such frameworks are below:
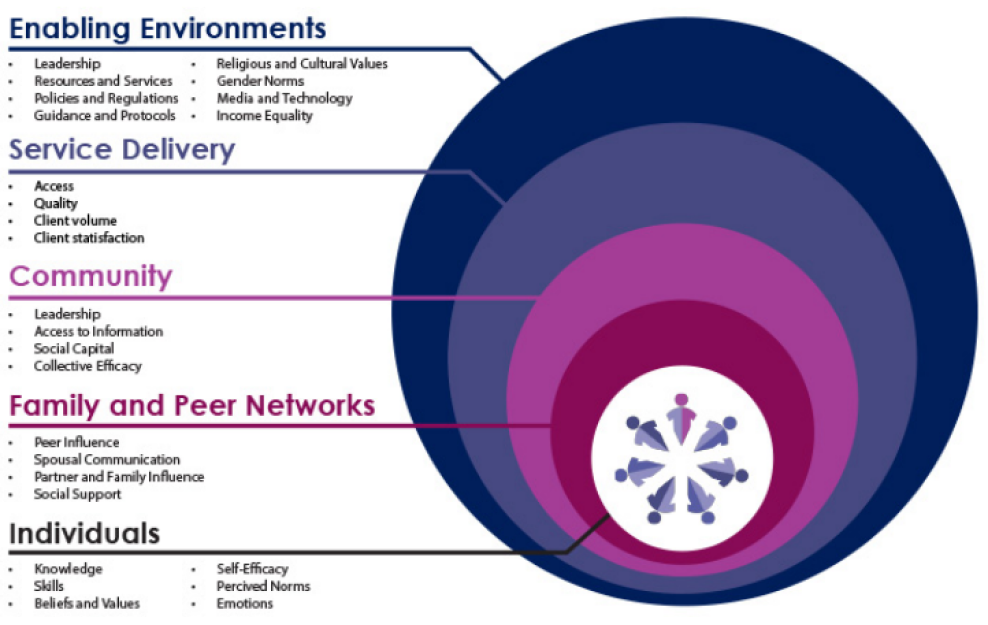
i) Socio-Ecological Model
A person’s behaviour is influenced by many factors both at the individual level and beyond. The levels of influence on behaviour can be summarized by the socio-ecological framework. This framework recognizes that behaviour change can be achieved through activities that target four levels: Individual, interpersonal (family/peer), community and social/structural.
ii) Gender Equality Continuum
Behaviour Change Communication programs generally fit along the Gender Equality Continuum (IGWG, 2013), which can be used as a planning framework or as a diagnostic tool. As a planning framework, it can be used to determine how to design and plan interventions that move along the continuum toward transformative gender programming. As a diagnostic tool, it can be used to assess if, and how well, interventions are currently identifying, examining and addressing gender considerations, and to determine how to move along the continuum toward more transformative gender programming.
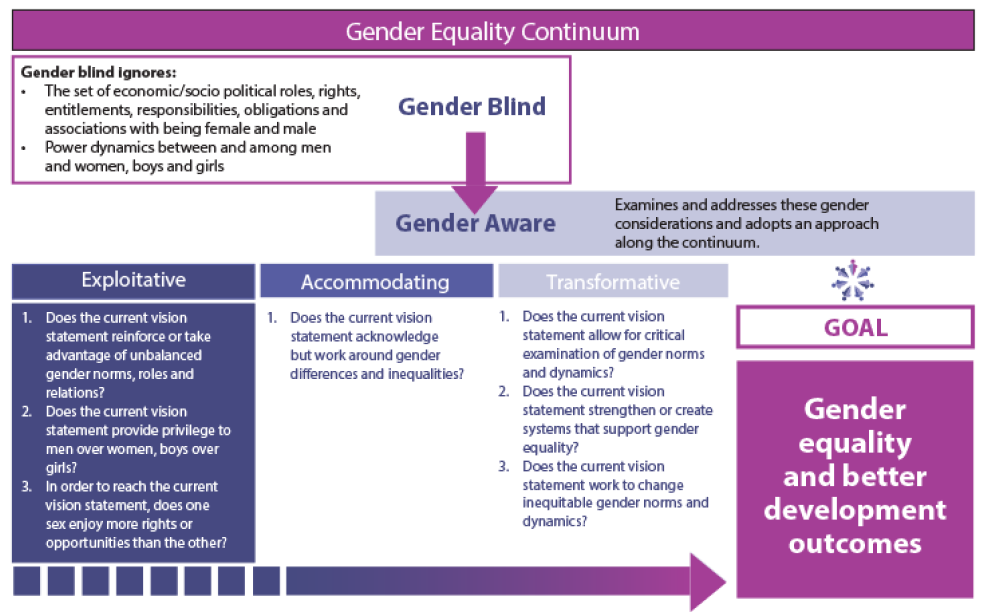
The continuum shows a process of analysis that begins with determining whether interventions are gender blind or gender aware. Gender blind policies and programs ignore gender considerations. They are designed without any analysis of the culturally defined set of economic, social and political roles, responsibilities, rights, entitlements, obligations and power relations associated with being female and male, or the dynamics between and among women and men, girls and boys.
Gender aware policies and programs examine and address the set of economic, social and political roles, responsibilities, rights, entitlements, obligations and power relations associated with being female and male, and the dynamics between and among women and men, and girls and boys.
The process then considers whether gender aware interventions are exploitative, accommodating or transformative.
While selecting from a number of such frameworks available, it is important to consider following:
A roundtable of public health practitioners was organized in November 2022, at New Delhi to initiate a discussion on gender barriers that impact health and nutrition outcomes and what platforms can and have been used to address these. Some of the discussion points are presented here. The consensus of the group was that all existing public health and nutrition guidelines must be looked at with a gender lens and gender mainstreaming interventions need to be included at the formative stage itself. The group identified some simple and doable actions that can be adopted to address current gaps.
5.1. Address the gaps in Policy and Planning at the highest levels:
Several barriers to realizing gender equity, are related to policy and planning. To ensure gender mainstreaming in upcoming and existing health programs, a gender Nodal officer, who is also a gender Champion is needed at the level of the relevant Ministry. This Officer would bring together experts to ensure that gender related relevant points are embedded in each policy and all programmatic components. To do this, some suggested critical actions were
5.2. Identify and address gaps in services using a gender norms lens:
This refers majorly to supply related issues that impact uptake of services by women. Women’s awareness and their participation in local governance as peer/social pressure groups can help alter gender norms and align health and nutrition supply with demand. Existing Women’s collectives / SHGs / other groups can serve as a platform for ensuring this.
i) Strengthen the Women’s Collective / SHG platform as a vehicle to bring about change in gender dynamics for health and nutrition in the household as well as community level. These collectives due to its strength of numbers and homogeneity are a critical source of social solidarity and resilience.
ii) Leverage women’s groups in filling the gaps for awareness on health and nutrition, access to services, streamlining of services and community follow-up/rehabilitation to reinstate women in better health.
iii) Anchor gender within the policy and governance of the country for gender integrated planning of HN services, emphasizing the need for convergence between departments, specifically making gender considerations essential and uniform.
iv) Promote convergence with PRIs and other platforms to engage men in conversations around gender and HN. This engagement should be built for a positive impact on addressing gender barriers that negatively impact the health and nutrition of women.
v) A learning collaborative of stakeholders can be formed for advocacy that could help in bringing priority on this subject. This will also help share and learn from each other since a lot of work is being done in this direction.
Authors: Archna Ghosh, Sushmita Mukherjee and Amrita Misra